Should it matter to Hoosiers that we have only one medical school in the state?
Yes, definitely, for at least two distinct reasons.
First, more medical schools would result in an increase in the number of physicians in the state which would in turn provide additional workforce capacity and opportunities to address medically underserved regions of the state.
Second, having more than one medical school in the state would lead to competition between or among the schools. Competition is one of the most reliable catalysts for innovation. A single medical school, as is true for many large organizations, tends to evolve toward a hierarchical organization structure that often becomes cumbersome and constrains the generation of new ideas. The challenges faced by a medical school that has a monopoly in a state is reminiscent of the challenges Christensen described in his book, “The innovators Dilemma.” [1] Nimbleness as a new organization can devolve into cumbersomeness as growth occurs.
As a medical school grows, unchallenged in a monopolistic environment, there is a danger that the very philosophy of teaching medicine and vigor of medical research will become stagnant and monochromatic as students, teachers, and researchers are inculcated with the institutional dogma that has developed unencumbered by effective, external competition.
There is a real concern that broad-based, innovating teaching methods and agile, pioneering medical research will be obtunded by a culture contaminated with a groupthink mindset.
The danger of a single medical school in a state is not necessarily a novel observation, nor is it limited to the United States. In his 2006 article, “Every Country or State Needs Two Medical Schools,” Adamson Muula opined, “A medical school that has a monopoly over health education in a country stands the real risk of accepting mediocrity.” [2]
Until Indiana finds the wherewithal to develop a second medical school, independent of Indiana University, Hoosiers will continue to pay the price of physician shortages and limited access to innovative care.
Only 16 states have only one medical school
According to data from the American Association of Medical Colleges [3], Indiana is only one of 16 states that have a single medical school. The others are Arkansas, Colorado, Hawaii, Iowa, Kansas, Mississippi, New Hampshire, New Mexico, North Dakota, Oregon, Rhode Island, South Dakota, Utah, Vermont, and Washington.
The perils of having only one medical school in a state has been the concern of the Washington Alliance of Teaching Physicians. Henry Mroch and Jeremy Graham of that organization wrote in a guest editorial of the Seattle Times, “Every year, about 250 promising, highly qualified students leave Washington, permanently in many cases, to attend medical school elsewhere. There simply are not enough seats in their own state to train them to fill Washington’s physician shortage. The solution is straightforward: Establish an additional medical school in Washington.” [4]
Geographically, Indiana is a single-medical-school island. All four states bordering Indiana have multiple medical schools. Kentucky has two (2), Michigan has six (6), Ohio has seven (7), and Illinois has nine (9). It would seem all our neighboring states know something that we Hoosiers have yet to grasp.
More medical schools, more physicians, better access to care
Indiana does have a shortage of physicians. According to the Indiana University Bowen Health Workforce Information Portal (HWIP), there only 29 counties in Indiana that are not designated as having either a county-wide or partial-county shortage of primary care physicians. The counties are identified in the map below available on the HWIP. [5]

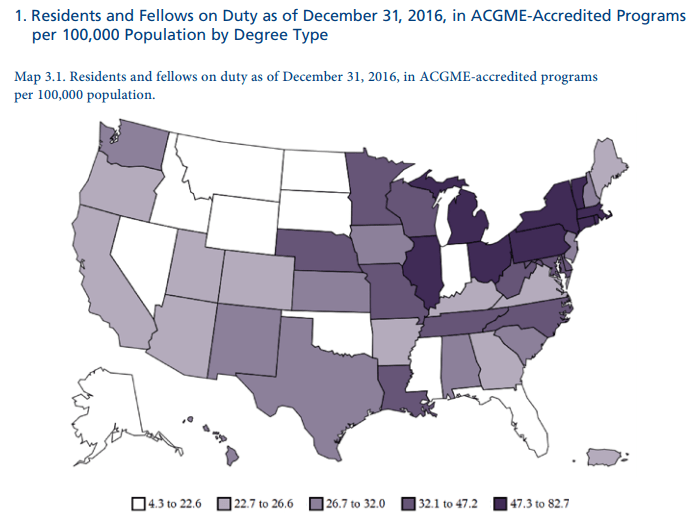
The basis of the shortage may be gleaned from the map below from the Stat News web page, “Explore: How many young doctors does your state retain after residency?” [6]
Train in Indiana, stay in Indiana
Graduates of medical schools tend to stay in states where they attended school. Increasing the number of medical schools in a state was a solution to help address physician shortages in Texas, California, and New Jersey. [7]
In Indiana, data from the HWIP shows that 39% of practicing primary care providers attended medical school in Indiana. [8]
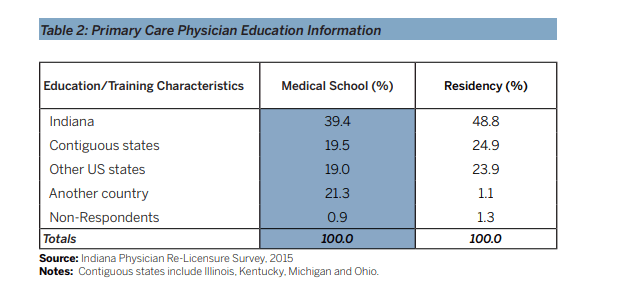
Source: Indiana University Bowen Health Workforce Information Portal
The tendency of Indiana medical graduates to remain in the state is also reflected in the map below. The bar chart following the map indicates that Indiana is above the national average in retaining medical school graduates. Both the map and bar chart are also from the State News web page referenced previously.

Source: Stat News

Source: Stat News
Increasing the number of medical school enrollees is a fundamental tenant of addressing the physician shortage. While it may be true enrollment could be increased by increasing the number of medical school campuses, that action would not address the more insidious and more challenging problem plaguing states with only one medical school – groupthink.
Groupthink is real
The term groupthink was first coined by Irving Janis in 1971. [9] He defined it as “a quick and easy way to refer to the mode of thinking that persons engage in when concurrence-seeking becomes so dominant in a cohesive ingroup that it tends to override realistic appraisal of alternative courses of action.”
Since that time, groupthink has been applied to multiple disciplines including large organization and medicine. At its core, a medical school is a large organization and is not immune from the pitfalls of groupthink. These pitfalls may be manifest in multiple areas such as a monolithic approach to teaching clinical care or a narrow focus on research topics.
For example, an institution that teaches that HDL/LDL ratios are the gold standard for managing lipids in patients may not be open to considering other factors as equally relevant. Similarly, research at medical schools is vulnerable to groupthink that causes a focus on diminishingly relevant research topics that are entrenched in the culture of the institution instead of applying resources to more current areas of research that may ultimately be of more benefit to patients.
In his book, Objectivity in Social Research, Gunnar Myrdal summarized this danger by stating, “Generally speaking, we can observe that the scientists in any particular institutional and political setting move as a flock, reserving their controversies and particular originalities for matters that do not call into question the fundamental system of biases they share.” [10]
Similar concerns about the adverse consequences of groupthink in a research environment were identified by Jain, et al, in Management of Research and Development Organizations: Managing the Unmanageable. The authors expressed their concern writing, “People often feel unjustifiably optimistic about the way their research plan will turn out, they do not give sufficient weight to signals that something is wrong, the reject those who criticize their plans or accomplishments, they censor themselves when they feel critical about the actions of their team members, and they select their critics so as to receive a favorable review of their work. All of these behaviors are aspects of groupthink. Groupthink leads to poor performance.” [11]
In Pediatrician’s Guide to Discussing Research with Patients, the authors identified the sunk cost logical fallacy as being another factor that negatively influences the agility of research at institutions. They write in chapter 2 of the book, “A bias affecting people who are involved in research projects spanning years is called the sunk cost fallacy. This bias exists because people do not make each decision in their lives independently of others they have already made. Instead, people perform something called “mental accounting,” in which they take their previous decisions into account when making a new one.” [12]
Institutions may not be aware they have fallen victim to the sunk cost fallacy or groupthink, writ large. In the words of Roland Bénabou, “… it often emerges that participants fell prey to a collective form of overconfidence and willful blindness: mounting warning signals were systematically ignored or met with denial, evidence avoided, cast aside or selectively reinterpreted, dissenters discouraged and shunned.” [13]
So, why not another medical school in Indiana?
The benefit to Hoosiers of having a second, independent medical school in the state is unambiguous. However, in order for a second medical school to come to fruition, a certain amount of cultural inertia must be overcome. Hoosiers may have come to conflate Indiana University with Indiana and may be reticent to support competition from a second school without Indiana in its name. One only need to observe the number of IU license plates to realize that demographics (of at least drivers) reflect strong support for anything IU.
This is not to disparage Indiana University or its alumni – I’m one of that group having undergraduate and graduate degrees from IU. One can still be a supporter of IU but also see the benefit of it having competition in the form of another medical school in the state.
The first step toward a second medical school is increased awareness that the status quo in Indiana is less than the status quo in states with multiple medical schools. It is not wrong for Hoosiers to want better access to care, broader medical research, and the ability to participate in a wider range of clinical trials. The last point is a topic for another post.
[1] http://www.claytonchristensen.com/books/the-innovators-dilemma/
[2] Muula AS. Every country or state needs two medical schools. Croat Med J. 2006;47(4):669-72. http://www.cmj.hr/2006/47/4/16909465.htm
[3] American Association of Medical Colleges data page, https://www.aamc.org/data
[4] Guest: Washington state needs another medical school, https://www.seattletimes.com/opinion/guest-washington-state-needs-another-medical-school/
[5] https://bowenportal.org/wp-content/uploads/2017/10/Primary-Care092517-StopLight.pdf
[6] https://www.statnews.com/2017/11/09/doctors-medical-residents-retention-rural/
[7] Texas could add 2 more medical schools, https://www.educationdive.com/news/texas-could-add-2-more-medical-schools/540766/
[8] 2016 Indiana Physician Licensure Survey, https://medicine.iu.edu/research/centers-institutes/bowen-health-workforce/#1495145103491-9a0eff16-11a3
[9] Janis, I. L. (1971). Groupthink. Psychology Today, 5, 43-46, 74-76. (PDF)
[10] Objectivity in Social Research (Pantheon Books, 1969, Page 53), https://www.amazon.com/Objectivity-Social-Research-Gunnar-Myrdal/dp/0394438841
[11] Management of Research and Development Organizations: Managing the Unmanageable, 2010, Page 37, Ravinder Kumar Jain, Raj Jain, Harry C. Triandis
[12] Pediatrician’s Guide to Discussing Research with Patients. 2017 Chapter 2, Page 20, https://library.villanova.edu/Find/Record/1640045/TOC (PDF)
[13] Groupthink: Collective Delusions in Organizations and Markets, 2008 Roland Bénabou, Princeton University (PDF)
