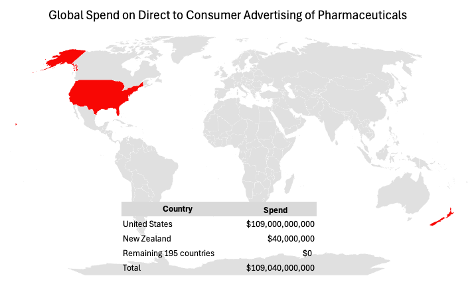
I first wrote about Direct To Consumer Advertising (DTCA)of pharmaceuticals in 2010 [1]. I wanted to revisit the topic to see if things had changed in 15 years. Not much, There are still only two countries in the world that allow DTCA – the United States and New Zealand. The US is responsible for 99.9% of the global spend on DTCA and New Zealand is a distant second a 0.1%.
Go to any other country in the world and you will not be bombarded by TV adds designed to induce viewers to leverage their doctors to prescribe a particular brand of pharmaceutical. Also, what hasn’t change is that DTCA works in terms of increasing profits for big pharma.
In 2024, one company, AbbVie, spent more than one billion dollars on DTCA – for two drugs.[2] The spend on Skyriza was 647 million and 553 million for Rinvoq. With an estimated total patient market of 2.2 million people [3] [4] [5] [6] [7] [8] [9] AbbVie sees the value in spending approximately $300 per potential patient per year. Of course, the reason they do that is because the cost of acquiring a new patient is far less than the lifetime value of that patient. Unarguably, they have become adept at manipulating consumers to pressure their doctors to prescribe their drugs.
Drug companies defend their DTCA as patient education but that belies the fact that it’s educating them in the questions to ask that result in more sales for them. But is DTCA good for patients in the United States? Not really. Non-DTCA countries deliver robust real-world outcomes for Skyrizi-treatable diseases—comparable to trial benchmarks and to U.S. practice—because outcomes are mainly a function of access, guidelines, and clinical management, not consumer ads.[10] And the case that DTCA itself improves health outcomes is weak; high-quality studies emphasize utilization and spending impacts rather than mortality or major morbidity gains. [11] Read those last two sentences again!
The bottom line is that consumers remain fertile ground for DTCA not because it improves health outcomes but because big pharma can make more money. That just doesn’t make sense to me. Maybe if I were invested in pharmaceutical companies it would.
[1] https://confrontingmediocrity.net/2010/08/21/dtca/
[2] https://www.fiercepharma.com/marketing/top-10-pharma-drug-ad-spenders-2024
[3] Rachakonda, T. D., Schupp, C. W., & Armstrong, A. W. (2014). Psoriasis prevalence among adults in the U.S. JAMA Dermatology, 150(7), 736–744.
[4] Takeshita, J., et al. (2017). Psoriasis severity distribution and burden. JAMA Dermatology, 153(12), 1127–1136.
[5] Dahlhamer, J. M., et al. (2016). Prevalence of IBD among adults—United States, 2015. MMWR, 65(42), 1166–1169.
[6] CDC. (2022). Inflammatory Bowel Disease (IBD) — Facts & Statistics. Centers for Disease Control and Prevention.
[7] Park, K. T., et al. (2020). Biologic utilization trends in IBD, 2011–2020. Inflammatory Bowel Diseases, 26(11), 1633–1641.
[8] Egeberg, A., et al. (2016). Association between psoriasis and IBD: A Danish nationwide study. Journal of Investigative Dermatology, 136(8), 1724–1730.
[9] Ungaro, R., et al. (2017). Psoriasis and risk of IBD: Systematic review & meta-analysis. Inflammatory Bowel Diseases, 23(3), 473–480.
[10] Thaçi, D., Ohtsuki, M., Maul, J.-T., Szegedi, A., Luna, P. C., Lynde, C. W., Soliman, A. M., Wang, H., Kaufmann, C., Ashley, D. G., Madihlaba, T., Rubant, S., & Papp, K. A. (2025). Real-world effectiveness of risankizumab in patients with moderate-to-severe psoriasis: Interim analysis from the VALUE global prospective post-marketing observational study at 25 months. Dermatology and Therapy, 15(2), 381–394. https://doi.org/10.1007/s13555-025-01342-0
[11] Weissman, J. S., Blumenthal, D., Silk, A. J., Zapert, K., Newman, M., & Leitman, R. (2003). Consumers’ reports on the health effects of direct-to-consumer drug advertising. Health Affairs (Millwood), Suppl Web Exclusives, W3-82–W3-95. https://doi.org/10.1377/hlthaff.w3.82
